On 26 February, Sydney Health Ethics, in partnership with InterAction for Health and Human Rights and PSI-I were delighted to host Dr Lih-Mei Liao at the University of Sydney for a very special event on psychosocial support for people with innate variations of sex characteristics (IVSCs, also known as intersex variations or differences of sex development).
More than 90 people with lived experience, academics and health professionals participated in the session, both in-person and online, to learn more about and discuss the importance of psychosocial support for people with innate variations of sex characteristics, with rich and thoughtful discussions in both online and in-person spaces. Participants also brainstormed possible solutions to increase the understanding, mainstreaming, and uptake of psychosocial care in clinical settings and beyond.
We would like to thank Dr Lih-Mei Liao, respondents Velissa Aplin (Canberra Health Services) and Bonnie Hart (InterLink/UniSQ), moderator/chair A/Prof Morgan Carpenter (USyd), the host for the online discussion, Prof Katrina Roen (Waikato), Sydney Health Ethics conversation series organiser Dr Supriya Subramani, and each of the partner organisations.
A recording of the event is available below, and you can learn more about the presenting and supporting event partners here.
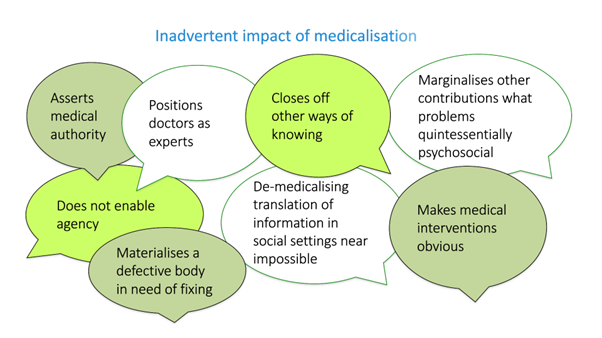
Lih-Mei delivered a keynote address on integrating psychosocial evidence to enhance modern healthcare for people with IVSCs. She outlined the history of the space, definitions, debates, impacts of medicalisation, and multidisciplinary teams and the under-utilisation of non-technical expertise.
Velissa Aplin offered the first response to Lih-Mei’s address, speaking to her experience as the Coordinator of the Variations in Sex Characteristics Psychosocial Service in the ACT. She highlighted the need for psychosocial support to be embedded and prioritised in healthcare for people with IVSCs, for legislation and reform processes to continue to be scaffolded and led, and noted that cultural change is happening – albeit slowly.
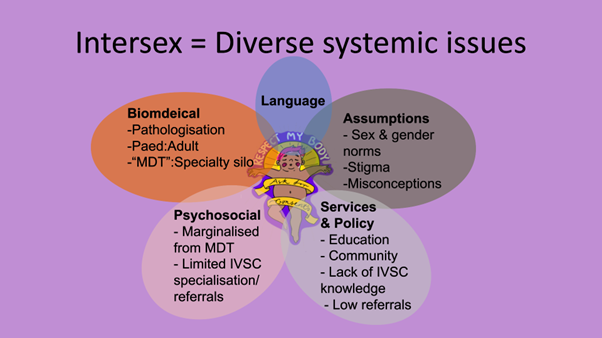
Bonnie Hart offered the second response, drawing upon her lived experience and positions as the Manager of InterLink and Deputy Executive Director of InterAction. She laid out the diverse system issues experienced by the IVSC population, including around psychosocial, biomedical, language, assumptions and services and policies, and spoke to the unique peer-led health and wellbeing services offered to the population and their families by InterLink.
Morgan Carpenter offered the final response, thanking speakers for their contributions and offering further context on the state of IVSC care in Australia, drawing on recent research on decision-making by paediatric multidisciplinary teams. This includes evidence from terms of reference that multidisciplinary teams in NSW and Victoria can meet without a psychologist, or without an ethicist.
Attendees then broke into groups to brainstorm how to best ensure clinical engagement with psychosocial frameworks, setting aside resourcing constraints. These rich discussions resulted in suggestions around the following thematic areas:
- How might we bring medical colleagues onboard? 1) Normalise psychosocial services/make benefit to broader medical treatment clear. 2) Top-down approach of making psychosocial care compulsory. 3) Culture and attitude change of ‘people in the room’.
- How might we bring parents onboard? 1) Resources made available from birth to support parents and normalise IVSCs and psychosocial support, including information available in baby bags / baby books for every parent, in antenatal clinics and fertility clinics. 2) Identify support pathways/first points of contact for parents to help facilitate/normalise access to psychosocial services. 3) A psychologist who has psychosocial expertise related to the IVSC population should be available in each hospital.
- What support is required for people at point of receiving a diagnosis? The first few moments are critical for people to learn about their body. A psychologist who has psychosocial expertise related to the IVSC population should be available in each hospital.
- How might we build understanding and capacity?: 1) comprehensive education in school across all forms of diversity. 2) Getting into medical schools’ curriculum, ensuring medical/nursing/allied health students have access to comprehensive information/teachings on IVSC issues that focus on the psychosocial. 3) Regulating Multidisciplinary Teams (MDTs) and ensuring they include lived-experience members who are remunerated and treated as professionals. 4) Ensuring that healthcare practitioners understand the role of psychosocial support and ensure that meaningful referrals happen. 5) Advocacy and policy work.
- What models could we look to implement? A national hub and spoke model that is well defined but flexible, that would be charged with supporting clinicians, families and individuals upon receipt of an IVSC diagnosis. This would include: 1) psychosocial experts in all key districts, and 2) a national panel comprised of lived experience psychosocial experts who are resourced to deliver modules on delivering care and supporting people with IVSCs in different ways.
- What resources are required? 1) Who will pay for large scale models and services? and how might the flow on benefits and cost savings (e.g., for hospitals) be best communicated? 2) For services, appropriate time and resourcing is required to recruit staff, train them, build relationships and understand the salience of local context. 3) To have real-world impact, well-resourced and meaningful co-design processes should be implemented in the development of clinical guidelines for the care of people with IVSCs.